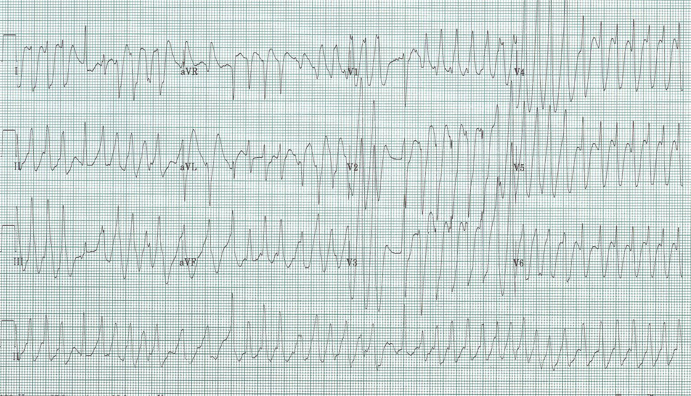
48-year-old man with palpitations and lightheadedness.
The rhythm is irregularly irregular with a wide-complex QRS – atrial fibrillation with aberrancy, pre-existing bundle, or conduction down a bypass tract of Wolfe-Parkinson-White syndrome. [see EKG Discussion regarding the differential of tachycardias on this website]
This rhythm is fairly uncommon but very important to recognize. Two features of this tachycardia strongly suggests involvement of a bypass tract – 1) the extremely rapid rate with R-R intervals at a rate of 300/minute or more, and 2) the varying morphology of the QRS complexes.
Treatment of this rhythm depends on the stability of the patient. If unstable, electrical cardioversion is always the right answer. This may require proceeding with defibrillation as the rapid complexes may not allow synchronized cardioversion.
Medical management is precarious because typical options for atrial fibrillation may cause deterioration of the rhythm causing ventricular fibrillation. Any medication that causes AV node blocking will increase conduction down the bypass tract often precipitating v. fib. So, avoid:
Adenosine
Beta-blockers
Calcium-channel blockers
Digoxin
Amiodarone has had a controversial recent history, with removal from the 2010 ACLS recommendation following multiple case reports of deterioration due to precipitation of ventricular fib. More recently expert opinions again endorse the use of amiodarone. Another acceptable alternative, and the board exam answer, is procainamide.