45-year-old man with 2 hours of chest pain and diaphoresis.
(Pay special attention to the rhythm strip).
Interpretation & Explanation
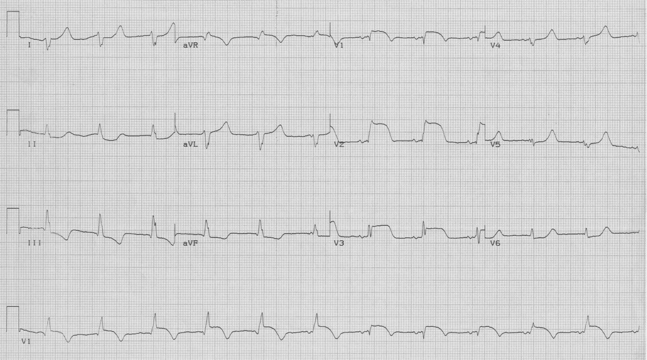
Looking at the V1 rhythm strip, the first five beats are an accelerated idioventricular rhythm (no P waves, wide complex, and regular rate of 70/minute). Just before the 6th beat you can see the “emergence” of a P wave – this particular P wave is very close to the subsequent QRS, and there is slight variation in the QRS morphology. The 6th QRS represents a fusion beat (a composite between the ventricular beat and a sinus-conducted beat occurring at nearly the same time). The 7th through 9th beats appropriately follow P waves and represent sinus conducted beats. This rhythm represents isorhythmic competition between accelerated idioventricular beats and sinus beats occurring at nearly the same rate.

The reason for this rhythm in this patient is apparent from leads V1-3 (the sinus conducted beats, so they can be interpreted) – the patient is having an acute anterior MI. Periods of accelerated idioventricular rhythm are common during acute infarction and especially during reperfusion following thrombolysis. AIVR has also been termed nonparoxysmal ventricular tachycardia or “slow v. tach”. It usually does not produce any hemodynamic change, and requires no specific treatment.