Elderly woman with generalized weakness x 2 days.
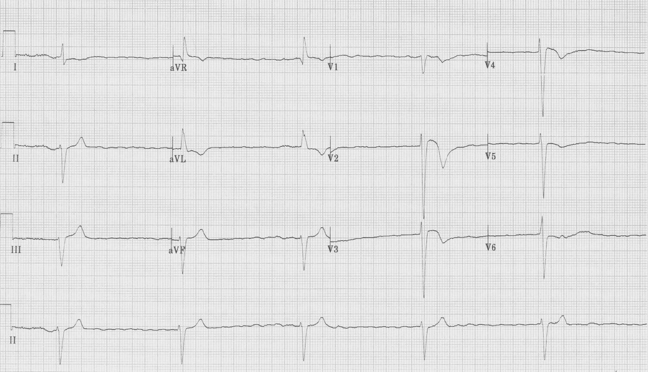
This EKG reveals a regular rhythm at 30/minute. There are no obvious P waves, although there appears to be irregular fine oscillations of the baseline, consistent with fibrillatory waves. Why would atrial fibrillation
present with a slow and regular ventricular response? Perhaps these ventricular beats are escape beats, occurring because the AV node is completely blocked! This is what complete heart block occurring with atrial fibrillation looks like…
If this patient was taking digoxin it would certainly be important to check a level to rule out toxicity. Digoxin toxicity classically causes two important EKG findings: 1) significant AV block (more than 1° AV block), and 2) increased automaticity (often accelerated junctional rhythm or atrial tachycardias). Typically these two EKG findings occur simultaneously – hence the classic dig toxic rhythms (PAT with block or “regularization” of the a fib due to 3° AV block with accelerated junctional escape rhythm).
PAT with 2:1 block (P waves at 150/minute – too slow for flutter waves, so these are discrete P waves and this is atrial tachycardia)

Another PAT (look hard for the P waves at 150/minute) with 2° AV block, type I

“Regularization of atrial fib” – due to accelerated junctional rhythm at 70/minute with 3° heart block of underlying a fib (note fibrillatory waves in V1)
